Salivary Gland Stones, Swellings and Surgery — What You Need to Know
- Vyas Prasad
- May 24
- 8 min read

Updated: 4 days ago
Salivary gland stones most commonly affect the submandibular gland, causing painful swelling at mealtimes
Most stones can now be removed through the natural duct using sialendoscopy — a minimally invasive technique requiring no external incision
Open surgery is no longer necessary in the majority of cases
This post explains the different glands affected, symptoms, and what treatment involves
Salivary gland stones most commonly affect the submandibular gland beneath the jaw, causing painful swelling at mealtimes that subsides between meals. Most stones can now be removed through the natural duct opening using sialendoscopy — a minimally invasive technique that preserves the gland and requires no external incision — making open surgery unnecessary in the majority of cases.
The salivary glands are among the least-discussed structures in the head and neck — until something goes wrong with them. A painful swelling under the jaw at mealtimes, a lump in front of the ear, or a persistently dry mouth can all point to a salivary gland problem. Most of the time these conditions are benign and highly treatable, but they do require accurate diagnosis to ensure the right treatment is chosen.
This article explains the most common salivary gland conditions, how they are investigated, and what treatment options are available — including the minimally invasive approach of sialendoscopy, which has transformed the management of salivary gland stones over the past two decades.
The Major Salivary Glands
There are three pairs of major salivary glands:
The parotid glands sit in front of and just below each ear, overlying the angle of the jaw. They are the largest salivary glands and drain into the mouth via a duct that opens opposite the upper back teeth. The facial nerve — the nerve controlling all movements of facial expression — passes directly through the parotid gland, which is an important consideration in any surgical procedure involving this gland.
The submandibular glands sit beneath the jawline on each side. They drain via a long duct (Wharton's duct) that runs forward and opens under the tongue. Because of this anatomy — a long duct with an uphill drainage pathway — the submandibular gland is by far the most common site for salivary gland stones.
The sublingual glands are the smallest pair, sitting in the floor of the mouth on either side of the tongue. They drain via multiple small ducts directly into the floor of the mouth.
There are also hundreds of minor salivary glands distributed throughout the lining of the mouth, lips, and throat.
Salivary Gland Stones (Sialolithiasis)
What Are Salivary Stones?
Salivary stones — sialoliths — are calcified deposits that form within the salivary ducts. They develop when minerals in saliva crystallise around a nidus of debris or mucus within the duct. They range in size from a grain of sand to, in rare cases, several centimetres.
Around 80% of salivary stones occur in the submandibular gland and its duct — a consequence of the gland's anatomy (long duct, uphill drainage) and the chemical composition of submandibular saliva (which is more alkaline and mucus-rich than parotid saliva, making it more prone to calcification).
What Are the Symptoms?
The hallmark of a salivary stone is mealtime pain and swelling. When you eat, your salivary glands are stimulated to produce saliva. If a stone is blocking the duct, saliva cannot drain freely — pressure builds behind the blockage, causing the gland to swell and become painful. The swelling typically peaks during or just after eating and gradually subsides over the following hour or two as saliva production decreases.
Symptoms include:
A painful swelling under the jaw (submandibular) or in front of the ear (parotid) at mealtimes
A visible or palpable lump that comes and goes
Dry mouth on the affected side
Occasionally, a visible white stone at the duct opening under the tongue or opposite the upper back teeth
If the blocked gland becomes infected — persistent swelling, tenderness, fever, and pus discharge from the duct opening
How Are Stones Diagnosed?
Clinical examination — palpating the duct and gland — can often identify a stone, particularly if it sits in the accessible anterior portion of the submandibular duct.
Imaging confirms the diagnosis and identifies the size and position of the stone:
Ultrasound is the first-line investigation and identifies most salivary stones
CT scan provides more detailed information about stone position, particularly for stones deep within the gland
Sialography (contrast X-ray of the duct) and MRI sialography are used in selected cases
Sialendoscopy — Minimally Invasive Stone Removal
Sialendoscopy has transformed the management of salivary gland stones. Before its development, many patients with stones required open surgery to remove the submandibular gland — a significant procedure with recovery time and a small risk to the surrounding nerves. Sialendoscopy allows most stones to be removed through the natural duct opening, without any external incision.
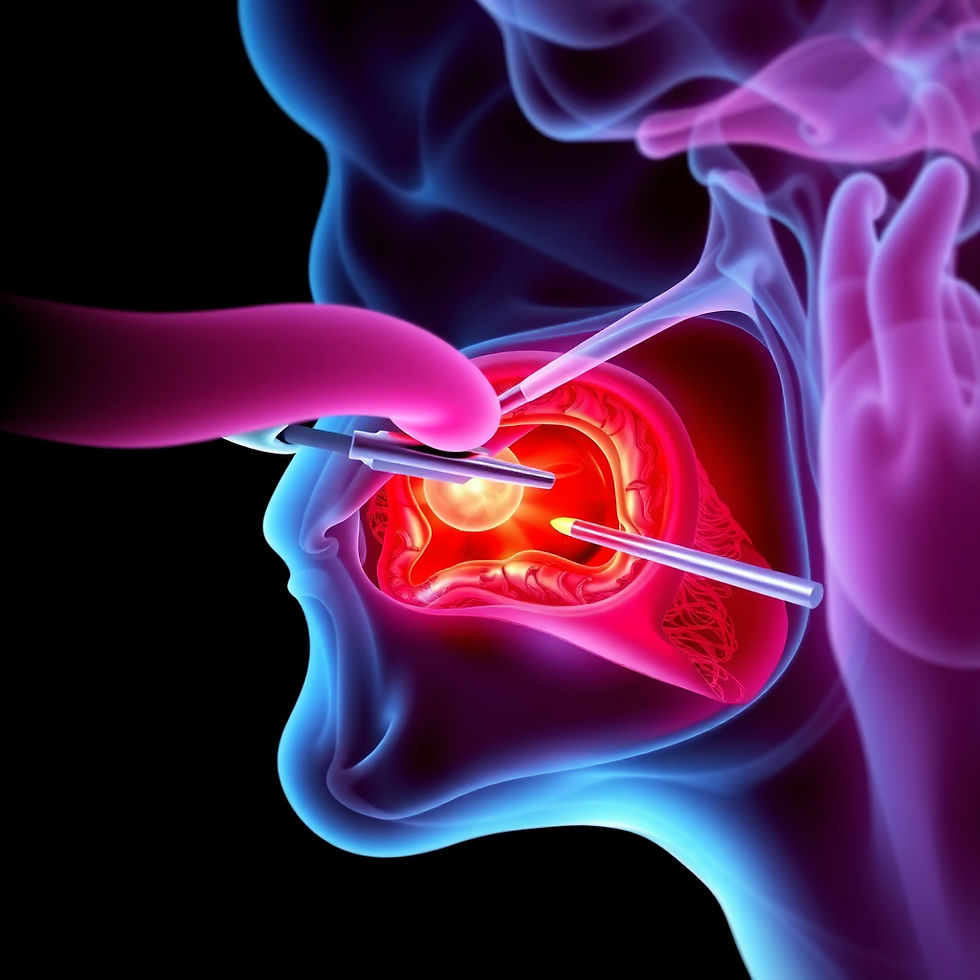
How Does It Work?
A tiny endoscope — thinner than a matchstick — is passed through the natural duct opening in the mouth. This allows direct visualisation of the duct interior. Once the stone is identified, fine instruments passed through the working channel of the endoscope are used to retrieve it. Larger stones may be fragmented first using a laser before retrieval.
What Are the Benefits?
No external incisions — no scar
The gland is preserved — function is maintained
Performed under general or local anaesthetic depending on stone size and position
Same-day or overnight procedure in most cases
Rapid recovery — most patients return to normal activities within a few days
When Is Sialendoscopy Suitable?
Sialendoscopy is appropriate for most stones within the duct. For very large stones within the gland substance itself, or where the gland has been irreversibly damaged by recurrent infection, gland removal may still be the more appropriate option. This is discussed on an individual basis after imaging review.
Salivary Gland Infections (Sialadenitis)
Acute Sialadenitis
Acute bacterial infection of a salivary gland most commonly occurs when a stone causes obstruction and stasis of saliva — creating conditions for bacterial overgrowth. It can also occur without a stone, particularly in debilitated or dehydrated patients.
The affected gland becomes swollen, tender, warm, and firm. Pus may be expressible from the duct opening. Treatment involves antibiotics, hydration, salivary stimulation (lemon drops, citric acid), and gentle massage of the gland. The underlying cause — usually a stone — should then be addressed to prevent recurrence.
Chronic Sialadenitis
Repeated episodes of acute infection, or prolonged partial obstruction, can lead to chronic inflammation and scarring of the gland. Chronic sialadenitis causes persistent or recurrent swelling, often without the acute pain of an infection. When the gland is significantly damaged and symptoms are significantly affecting quality of life, removal of the gland may be the best long-term solution.
Viral Parotitis (Mumps)
Mumps — caused by the paramyxovirus — causes acute bilateral parotid swelling in unvaccinated individuals. It is now uncommon in Singapore due to routine childhood vaccination. Viral parotitis is managed supportively.
Salivary Gland Tumours
How Common Are They?
Salivary gland tumours are uncommon but important to recognise. They most frequently arise in the parotid gland — which, being the largest salivary gland, is also the most common site overall. Around 80% of parotid tumours are benign. In the submandibular and minor salivary glands, the proportion of malignant tumours is higher.
Benign Tumours
Pleomorphic adenoma is the most common salivary gland tumour — a slow-growing, painless, firm lump that typically presents in the parotid in middle-aged adults. Despite being benign, pleomorphic adenomas require surgical removal because they can undergo malignant transformation over time if left untreated, and because they tend to recur if not removed with an adequate margin of surrounding tissue.
Warthin's tumour is the second most common benign parotid tumour, occurring almost exclusively in the parotid and with a strong association with smoking. It is sometimes bilateral. Surgical removal is the treatment of choice.
Malignant Tumours
Malignant salivary gland tumours — including mucoepidermoid carcinoma, adenoid cystic carcinoma, and acinic cell carcinoma — are less common but require prompt assessment and multidisciplinary management. Features that raise concern for malignancy include rapid growth, pain, facial nerve weakness, skin fixation, and cervical lymph node enlargement.
Assessment of a Salivary Gland Lump
Any persistent parotid or submandibular swelling should be assessed. Investigation typically includes:
Ultrasound to characterise the lesion
Fine-needle aspiration cytology (FNAC) to sample cells for analysis — a quick, well-tolerated in-clinic procedure
MRI for detailed characterisation of complex or deep lesions
Parotid Surgery
Surgery on the parotid gland — parotidectomy — requires specific expertise because the facial nerve passes directly through the gland. Identifying, tracing, and preserving this nerve throughout the procedure is the central technical challenge of parotid surgery.
A superficial parotidectomy — removing the superficial lobe of the gland where most tumours arise — is performed through a carefully placed incision in front of and below the ear. In experienced hands, the risk of permanent facial nerve weakness is low, though temporary weakness in the immediate post-operative period is not uncommon and usually resolves fully.
Total parotidectomy — removing both lobes — is performed when tumours extend into the deep lobe, or in the management of malignant parotid tumours.
Submandibular Gland Removal
When the submandibular gland requires removal — for a large stone within the gland, chronic sialadenitis, or a tumour — the operation is performed through a small incision beneath the jawline. The key structures to protect during this procedure are the marginal mandibular branch of the facial nerve (which controls the lower lip), the hypoglossal nerve (tongue movement), and the lingual nerve (tongue sensation).
Recovery typically involves one to two days in hospital and one to two weeks of reduced activity.
The scar sits in a natural skin crease and heals well.
Frequently Asked Questions
Will I produce less saliva if a salivary gland is removed?
The remaining salivary glands compensate well in most patients. Significant dry mouth is uncommon after removal of a single gland, though some patients notice mild dryness particularly when eating. Staying well hydrated and using salivary stimulants where needed helps.
Can salivary stones come back after sialendoscopy?
New stones can form in a small proportion of patients after stone removal. The risk is reduced by staying well hydrated and maintaining good oral hygiene. If symptoms recur, repeat sialendoscopy is usually possible.
Is a parotid lump always serious?
No — the majority of parotid lumps are benign. However, all persistent parotid swellings should be assessed and investigated, as the minority that are malignant are best treated early.
How long is recovery after parotid surgery?
Most patients stay one night in hospital and take one to two weeks off work. The wound is closed with dissolvable sutures or skin clips. Temporary numbness of the earlobe — due to the great auricular nerve — is common and usually recovers over several months. Flushing or sweating over the parotid area when eating (Frey's syndrome) is a recognised late complication that occurs in a proportion of patients.
Is salivary gland surgery covered by Medisave in Singapore?
Surgical procedures for salivary gland conditions — including sialendoscopy, parotidectomy, and submandibular gland removal — are generally claimable under Medisave and most integrated shield plans when performed for medical indications. The clinic team can assist with pre-authorisation.
Book a Salivary Gland Assessment
If you have a swelling under the jaw or in front of the ear, pain at mealtimes, or have been told you have a salivary gland stone or lump, a specialist assessment can clarify the diagnosis and guide the most appropriate treatment.
Dr Vyas Prasad consults at Absolute ENT, Camden Medical Centre, 1 Orchard Boulevard, #09-08, Singapore. Contact the clinic by WhatsApp on +65 8060 8079 or by email at camden.mmc@gmail.com.


Comments