Thyroid Cancer Surgery: What to Expect from Consultation to Recovery
- Vyas Prasad
- Apr 9
- 9 min read

Updated: 4 days ago
Thyroid cancer is one of the most treatable cancers when identified early, and surgery — thyroidectomy — is the primary treatment for most types. The key surgical considerations are complete removal of the affected tissue, preservation of the recurrent laryngeal nerve controlling voice, and protection of the parathyroid glands regulating calcium — all areas where subspecialty ENT head and neck surgical expertise makes a significant difference to outcomes.
Thyroid cancer is one of the most treatable cancers when diagnosed early — surgery is the primary treatment
The extent of surgery (total vs. partial thyroidectomy) depends on the cancer type, size, and risk profile
Key considerations include voice and parathyroid preservation, and whether radioiodine treatment will follow
Recovery is generally straightforward and most patients return to normal activity within weeks
A diagnosis of thyroid cancer is frightening, and the prospect of surgery adds another layer of anxiety. One of the most important things I try to convey to patients at the outset is this: thyroid cancer is one of the most treatable cancers we know of. For the majority of patients — particularly those with papillary or follicular thyroid cancer, which together account for around 90 percent of cases — surgery is highly effective, outcomes are excellent, and the disruption to normal life, while real, is typically measured in weeks rather than months.
What makes a meaningful difference to outcomes — and to the patient's experience — is having surgery performed by a surgeon with specific expertise in thyroid and head and neck surgery, who understands the anatomy in detail and has the skill to protect the structures at risk. This article explains what the process involves, from the initial consultation through to recovery, so that patients facing thyroid surgery know what to expect at each stage.
The Initial Consultation
The first consultation has two purposes: to establish the diagnosis with confidence, and to begin the process of planning the right operation.
By the time most patients see me, they will already have had some investigation — a thyroid ultrasound, and often a fine needle aspiration cytology (FNAC) result. I review all available imaging and pathology in detail before the consultation, so that we can have a genuinely informed discussion rather than simply repeating tests that have already been done.
During the consultation, I will:
Take a full history, including any symptoms such as a lump in the neck, voice change, difficulty swallowing, or pain
Examine the neck carefully, assessing the thyroid and the lymph nodes
Review the ultrasound and FNAC findings, and explain what they mean in plain terms
Arrange any further investigation needed — this may include additional imaging (CT or MRI of the neck and chest), repeat FNAC, or molecular testing of the biopsy sample if the result was indeterminate
Discuss whether surgery is recommended, what type of operation is most appropriate, and what the alternatives are
I encourage patients to bring a family member or friend to this appointment. It is a great deal of information to absorb, and having a second pair of ears helps. I also encourage patients to write down questions in advance — there are no questions too small or too obvious.
Understanding the Surgical Options
The extent of surgery depends on the type and stage of thyroid cancer, the size and location of the tumour, whether lymph nodes are involved, and the patient's individual circumstances.
Total thyroidectomy
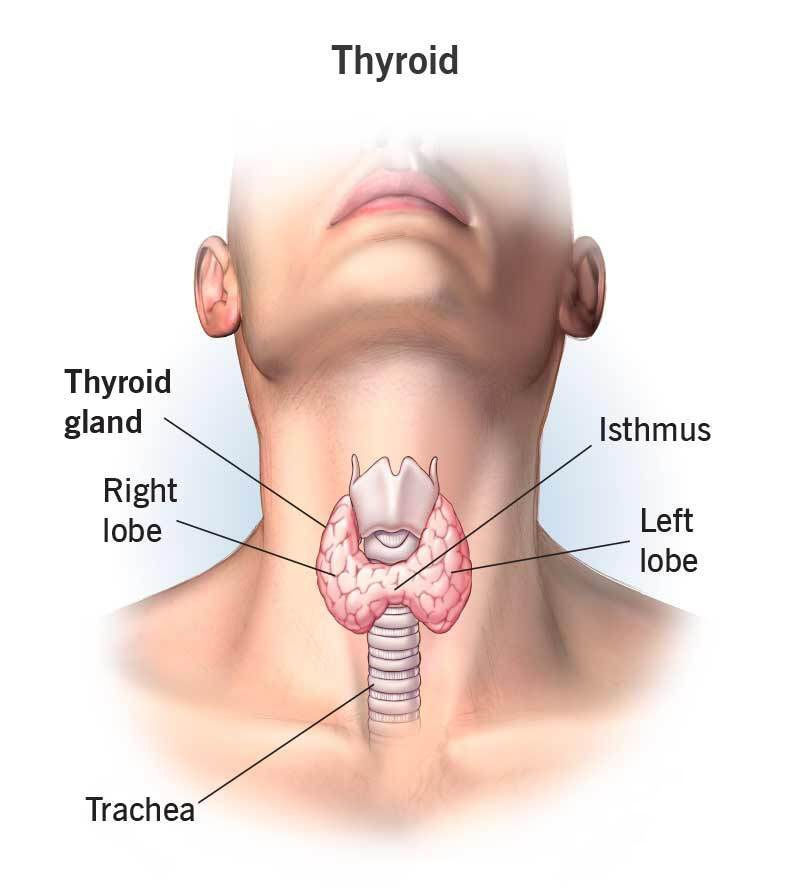
For most thyroid cancers — particularly those that are larger, bilateral, aggressive in type, or associated with lymph node involvement — total thyroidectomy is the standard approach. The entire thyroid gland is removed through a small, carefully placed incision in the lower neck. The operation preserves the four parathyroid glands (which regulate calcium) and both recurrent laryngeal nerves (which control vocal cord movement) — structures that lie in close proximity to the thyroid and require meticulous surgical technique to protect.
Following total thyroidectomy, patients take lifelong thyroid hormone replacement — levothyroxine — which is a tablet taken once daily. This is straightforward to manage and most patients adjust to it without difficulty.
Hemithyroidectomy (lobectomy)
For smaller, low-risk cancers — particularly small papillary cancers confined to one lobe without lymph node involvement — removal of the affected lobe alone (hemithyroidectomy) may be appropriate. This is a slightly smaller operation with a lower risk of affecting the parathyroid glands, and a proportion of patients retain enough residual thyroid function not to require hormone replacement.
The decision between total thyroidectomy and hemithyroidectomy is nuanced and depends on the specific characteristics of each patient's cancer. I discuss this in detail at consultation, including the implications for surveillance and the likelihood of needing additional treatment.
Neck dissection
If the cancer has spread to lymph nodes in the neck — either confirmed on imaging or discovered during surgery — a neck dissection is performed at the same time as the thyroidectomy. This involves systematic removal of the lymph nodes in the affected compartment of the neck. A central neck dissection removes nodes in the central compartment (between the carotid arteries, in front of the trachea); a lateral neck dissection addresses nodes along the jugular vein on one or both sides.
Neck dissection adds some complexity to the operation and recovery but is an important part of achieving complete surgical clearance.
The Consent Process
Before any operation, I conduct a thorough consent discussion — not a form-signing exercise, but a genuine conversation about what the surgery involves, what it is intended to achieve, and what the risks are. I believe patients make better decisions and recover better when they go into surgery with a clear and honest understanding of what to expect.
The key risks specific to thyroid surgery are:
Voice change — recurrent laryngeal nerve injury
The recurrent laryngeal nerve runs in close proximity to the thyroid on both sides and controls the movement of the vocal cords. Temporary voice change — hoarseness or weakness — occurs in a small proportion of patients as the nerve recovers from the handling it experiences during surgery. Permanent nerve injury, resulting in lasting vocal cord paralysis, is uncommon in the hands of an experienced thyroid surgeon but is a real risk that must be discussed honestly.
I use intraoperative nerve monitoring (IONM) routinely during thyroid surgery — a system that allows real-time assessment of nerve function throughout the operation, helping to identify and protect the nerve at every stage. This significantly reduces the risk of nerve injury.
If voice change does occur postoperatively, it is assessed promptly by laryngoscopy. In most cases of temporary paresis, the voice recovers fully within weeks to months. Where permanent paralysis occurs, effective treatments exist to restore voice quality — including vocal cord injection and thyroplasty procedures that I am trained to perform.
Low calcium — hypoparathyroidism
The four parathyroid glands, which regulate calcium levels in the blood, are closely associated with the thyroid and are at risk during thyroidectomy. Temporary low calcium — causing symptoms such as tingling in the fingers or around the mouth — is relatively common in the first few days after total thyroidectomy and is managed with calcium and vitamin D supplementation. In the majority of cases, parathyroid function recovers fully within weeks to months.
Permanent hypoparathyroidism — where calcium supplementation is required indefinitely — occurs in a small minority of patients and is more likely where the surgery is extensive or the parathyroid glands are poorly vascularised. Calcium levels are monitored closely after surgery and supplementation is adjusted accordingly.
Bleeding
A haematoma — a collection of blood in the wound — is an uncommon but potentially serious complication of thyroid surgery, because of the confined space of the neck. If significant bleeding occurs in the first hours after surgery, prompt return to theatre is required to evacuate the haematoma and secure the bleeding point. The risk of this complication is low — around 1 to 2 percent — and is reduced by meticulous surgical technique and careful postoperative monitoring.
Scar
All thyroid surgery leaves a scar in the lower neck. I place the incision carefully within a natural skin crease, where it heals to become well-concealed and fades significantly over the months following surgery. Most patients are satisfied with the cosmetic outcome. Scar care advice is provided after surgery.
The Operation Itself
Thyroid surgery is performed under general anaesthesia, typically taking two to three hours depending on the extent of the procedure. Patients are asked not to eat or drink from midnight the night before.
In the operating theatre, the neck is extended gently to improve access. A small incision — usually three to five centimetres — is made in the lower neck along a skin crease. The thyroid gland is carefully dissected from the surrounding structures, with continuous nerve monitoring used to identify and protect the recurrent laryngeal nerves. The parathyroid glands are identified and preserved with their blood supply wherever possible.
Once the thyroid — or the relevant lobe — has been removed, the specimen is sent for histological analysis. The wound is closed in layers, and a small drain is sometimes placed to prevent fluid accumulation overnight. The entire procedure is performed with the aim of leaving a clean, small, well-healed scar.
After Surgery: The First 24 to 48 Hours
Most patients undergoing total thyroidectomy stay one to two nights in hospital. After a hemithyroidectomy, a single overnight stay or even day-case surgery may be appropriate depending on individual circumstances.
In the immediate postoperative period:
Pain is typically mild to moderate and well controlled with simple analgesics. Significant pain is uncommon and should be reported
The voice may sound slightly different — softer, huskier, or fatigued — in the first days, which is normal. Significant hoarseness warrants prompt assessment
Calcium levels are checked on the morning after surgery and again before discharge. Calcium supplements are prescribed routinely after total thyroidectomy
The drain, if present, is removed the morning after surgery once drainage has reduced to a minimal level
Swallowing is usually comfortable from the day of surgery. A soft diet for the first day or two is generally recommended
Recovery at Home
Most patients feel well enough to return to light activity — working from home, gentle walking, and routine daily tasks — within one to two weeks. More physically demanding work or exercise is typically resumed at three to four weeks, depending on progress.
Voice — any hoarseness present at discharge usually improves steadily over the weeks following surgery. I arrange a laryngoscopy at the six-week mark to assess vocal cord movement directly. Patients with demanding voice requirements — professional singers, teachers, barristers — are referred to a specialist speech and language therapist for voice rehabilitation if needed.
Calcium — calcium and vitamin D supplements are gradually reduced as parathyroid function recovers, guided by blood test results at two and six weeks after surgery.
Levothyroxine — after total thyroidectomy, thyroid hormone replacement is started within the first one to two days after surgery. The dose is adjusted based on blood tests at six weeks and again at three months until the TSH level is in the target range for the specific cancer type.
Wound care — the wound is kept dry for the first week. After suture or clip removal at around ten days, silicone scar gel or strips can be used to optimise healing. Sun protection over the scar is recommended for the first year.
Follow-Up and Surveillance
Thyroid cancer follow-up is structured and ongoing. The specifics depend on the cancer type, stage, and whether radioactive iodine (RAI) treatment is recommended after surgery.
Radioactive iodine
For many patients with papillary or follicular thyroid cancer, a course of radioactive iodine is recommended after total thyroidectomy. RAI is taken as a capsule or liquid and is absorbed selectively by any residual thyroid tissue or cancer cells — it does not affect other organs. A period of thyroid hormone withdrawal or recombinant TSH stimulation is required beforehand to maximise uptake. RAI treatment is coordinated with the nuclear medicine team.
Blood tests
Thyroglobulin — a protein produced by thyroid cells — is used as a tumour marker after surgery. In patients who have had a total thyroidectomy and RAI, thyroglobulin should be undetectable. Rising levels may indicate recurrence and prompt further investigation. TSH is monitored to ensure hormone replacement is at the appropriate level.
Imaging
Neck ultrasound is performed at six to twelve months after surgery and periodically thereafter to monitor the lymph nodes for recurrence. Further imaging — CT, PET, or whole-body RAI scan — is arranged if there is any clinical concern.
Questions to Ask Before Your Surgery
Which type of thyroid cancer do I have, and how does that influence the operation?
Do I need a total thyroidectomy, or is a hemithyroidectomy appropriate?
Will you be using nerve monitoring during my surgery?
What is the likelihood I will need radioactive iodine after surgery?
How long will I need to take calcium supplements?
What follow-up will I need, and for how long?
What should I do if my voice changes significantly after surgery?
Facing thyroid surgery? Dr Vyas Prasad is a fellowship-trained thyroid surgeon at Camden Medical Centre — contact us to discuss your case.
Taking the Next Step
If you have been diagnosed with thyroid cancer, or have a thyroid nodule under investigation, I would be glad to see you at Camden Medical Centre for a specialist surgical opinion. I work closely with endocrinologists, radiologists, and the nuclear medicine team to ensure every patient receives a fully coordinated, personalised plan — from the first consultation through to long-term follow-up.
Please contact us to arrange an appointment.


Thank you for the great blog post
Was operated by Dr Vyas for thyroid cancer- this information is vital to anyone who is diagnosed with thyroid cancer and requires treatment. Thank you Dr Vyas.
Thorough but succinct and educational
Informative